Key Takeaway
Meta-analysis with trial sequential analysis of 16 RCTs (2,130 patients) found IV vitamin C monotherapy significantly reduced overall mortality in critically ill patients (RR 0.73), with greatest benefit in higher-risk populations.
Summary
Systematic review and meta-analysis with trial sequential analysis (TSA) evaluating intravenous vitamin C (IVVC) monotherapy in adult critically ill patients. The study searched four databases from inception through June 2022 without language restrictions, specifically isolating the effect of vitamin C alone (excluding combination therapies like thiamine-hydrocortisone protocols).
Sixteen RCTs with 2,130 participants were included. The primary outcome showed that IVVC monotherapy was associated with a significant reduction in overall mortality (risk ratio 0.73, 95% CI 0.60-0.89, p = 0.002, I-squared = 42%). Subgroup analysis revealed the greatest benefit in trials enrolling patients with baseline mortality above 37.5% (RR 0.65), suggesting high-acuity patients benefit most.
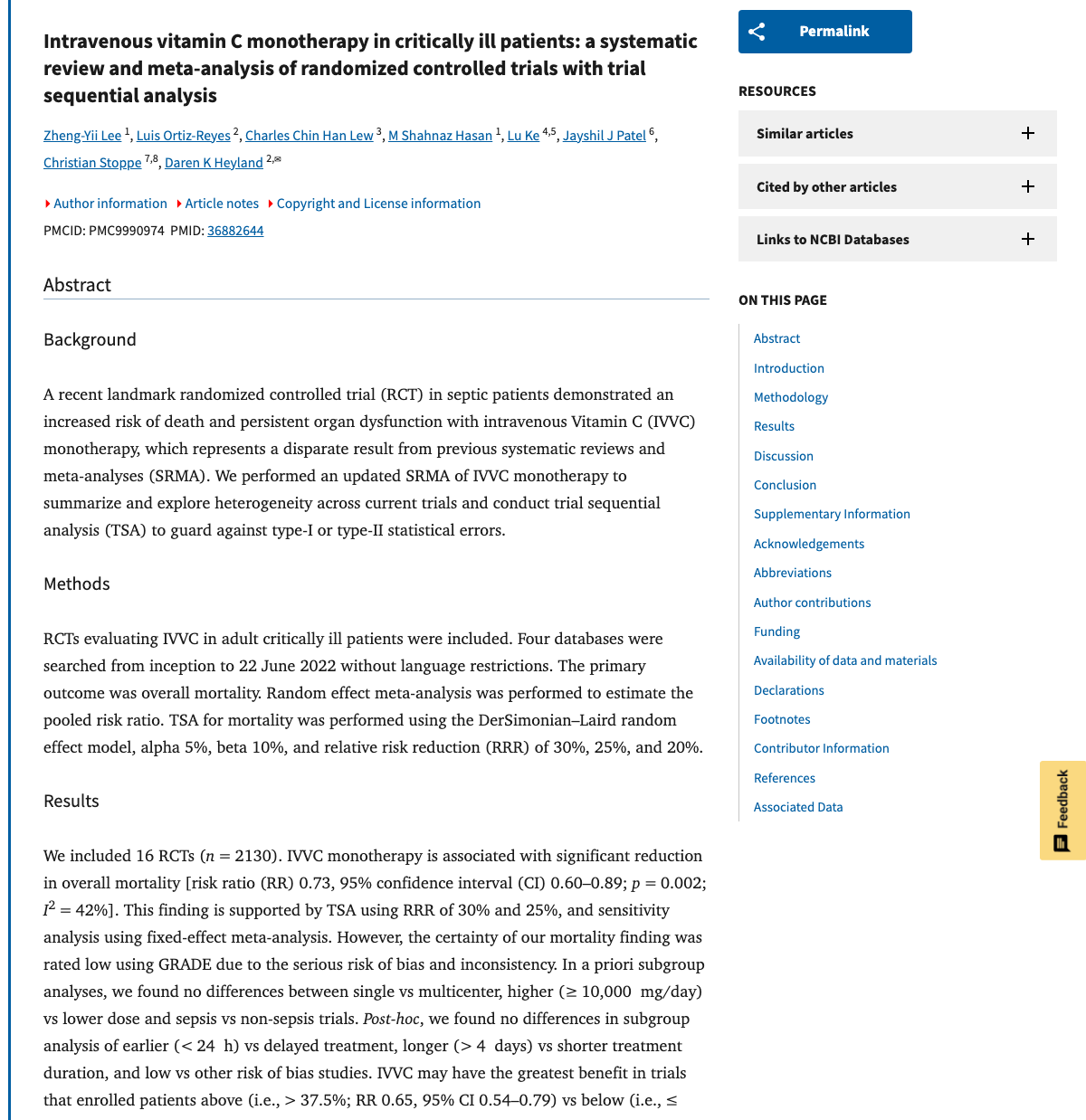
Trial sequential analysis was conducted to account for the risk of random errors from repeated significance testing. The analysis used specific parameters (alpha 5%, beta 10%, relative risk reductions of 30%, 25%, and 20%). Despite the positive mortality signal, the certainty of evidence was rated low by GRADE criteria due to serious risk of bias and inconsistency among studies. The authors concluded that further research is needed to determine optimal timing, dosage, treatment duration, and patient selection.
Methods
- Systematic review and meta-analysis with trial sequential analysis
- Searched four databases from inception to June 2022
- 16 RCTs with 2,130 participants included
- Random-effects meta-analysis
- GRADE assessment of evidence certainty
- TSA parameters: alpha 5%, beta 10%, RRR 20-30%
- Focused on IVVC monotherapy (excluded combination protocols)
Key Results
- Significant reduction in overall mortality (RR 0.73, 95% CI 0.60-0.89, p = 0.002)
- Moderate heterogeneity (I-squared = 42%)
- Greatest benefit in higher-risk populations (baseline mortality > 37.5%: RR 0.65)
- Trial sequential analysis supported the mortality reduction finding
- IVVC monotherapy isolated from confounding combination therapies
Figures
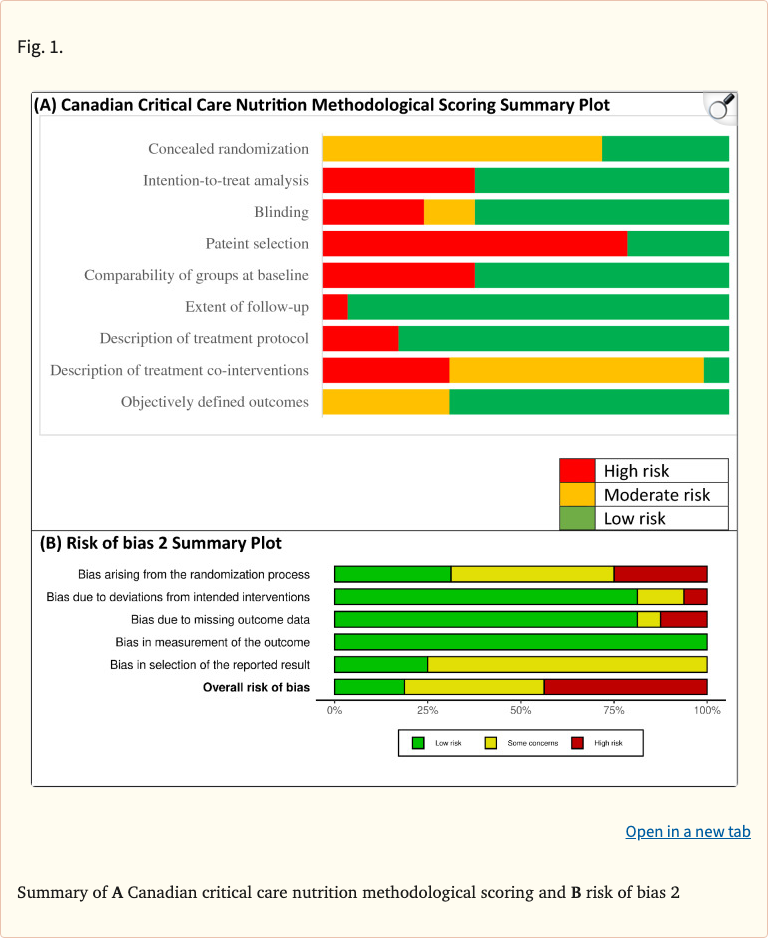 Figure 1
Figure 1
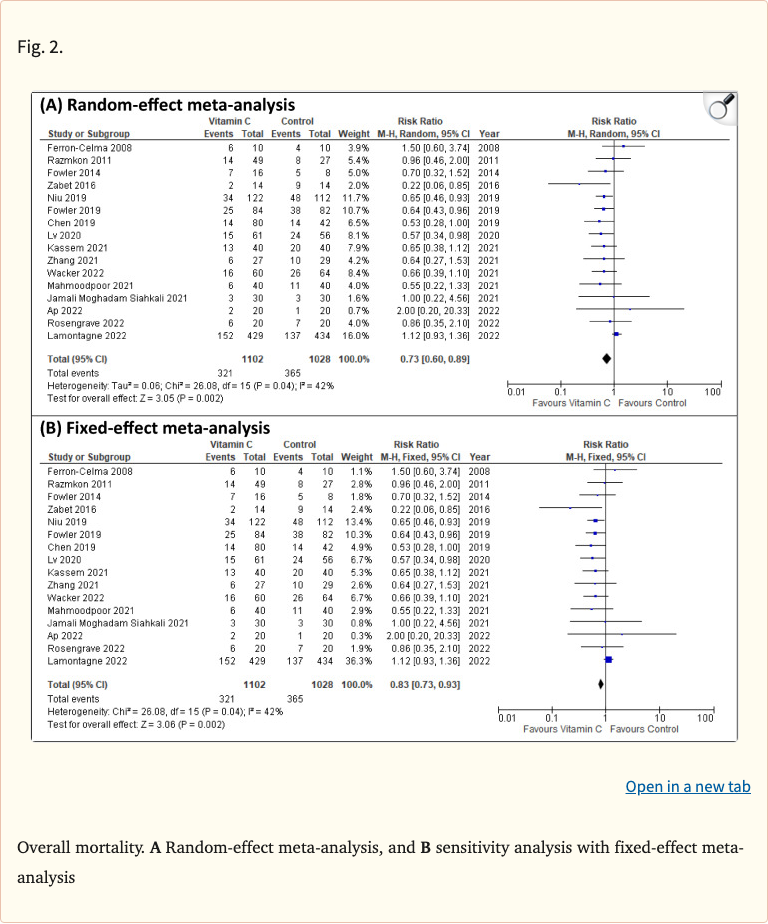 Figure 2
Figure 2
 Figure 3
Figure 3
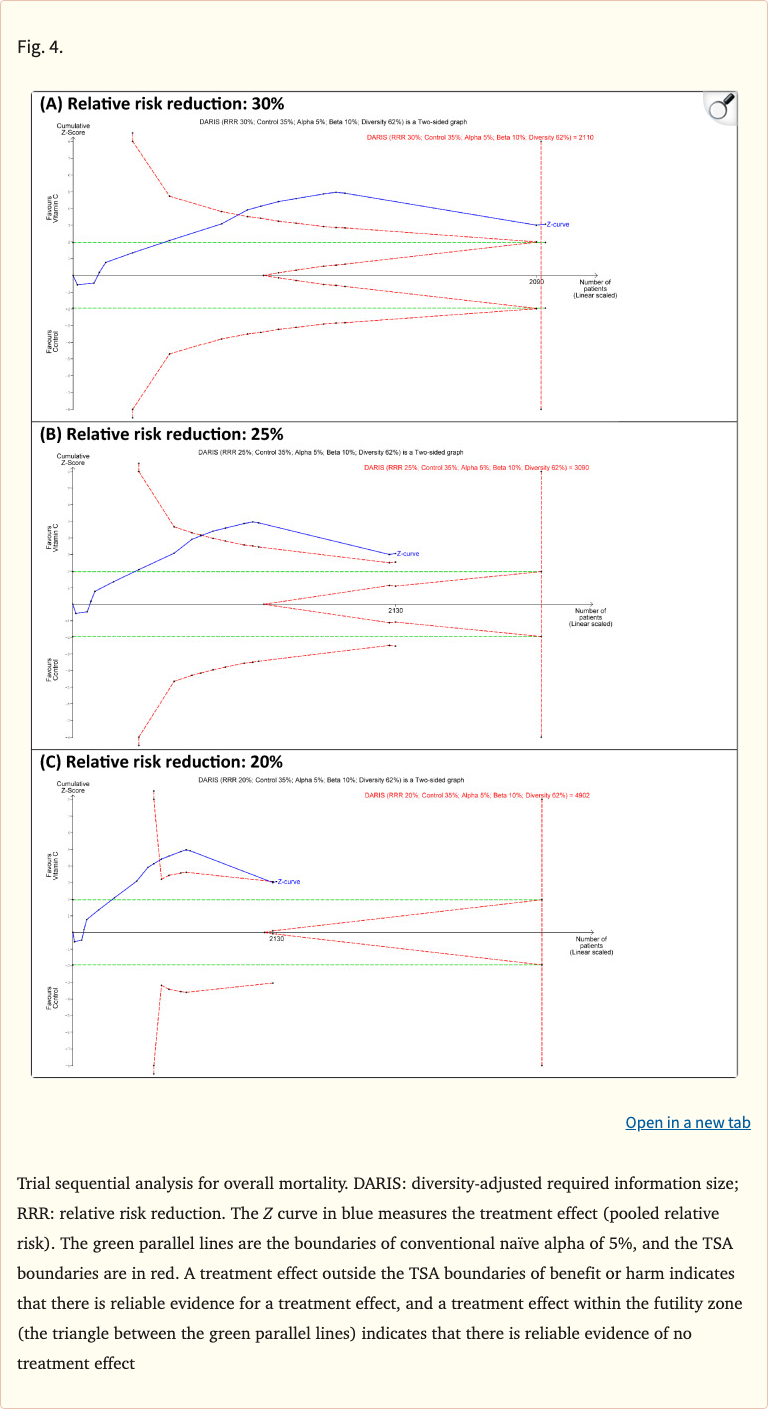 Figure 4
Figure 4
Limitations
- Low certainty of evidence by GRADE (risk of bias, inconsistency)
- Heterogeneity in dosing, timing, and duration across trials
- Optimal patient population not definitively established
- Variable ICU settings and illness severity
- Need for further large, well-designed RCTs to confirm findings