Key Takeaway
Spinal manipulation provides modest short-term improvements in pain and function for acute low back pain, with effects comparable to other recommended conservative treatments
Summary
This systematic review and meta-analysis published in JAMA evaluated spinal manipulative therapy for acute low back pain (less than 6 weeks duration). The authors conducted comprehensive searches of multiple databases and included 26 randomized controlled trials.
Results showed that SMT was associated with modest improvements in pain (approximately 10 points on a 100-point visual analog scale) and function in the short term. The quality of evidence ranged from low to moderate. Benefits were primarily seen in the first 6 weeks, with no clear long-term superiority over other treatments.
The findings support SMT as one reasonable option among several for acute low back pain, but do not suggest it is superior to other recommended conservative approaches like NSAIDs or exercise.
Methods
Systematic review and meta-analysis searching PubMed, EMBASE, Cochrane Library, and other databases through 2016. Included 26 RCTs of adults with acute low back pain (<6 weeks). Assessed SMT including high-velocity low-amplitude thrust techniques. Used GRADE framework for evidence quality. Outcomes included pain (VAS 0-100) and functional status. Risk of bias assessed using Cochrane criteria.
Key Results
SMT was associated with statistically significant improvements in pain (mean difference -9.95 on 100-point scale, 95% CI -15.6 to -4.3) and function at up to 6 weeks. Quality of evidence was moderate for pain and low for function. No serious adverse events were reported across included trials. Benefits diminished at longer follow-up periods, with no significant differences at 3 or 6 months. Effect sizes were modest and comparable to other recommended treatments.
Figures
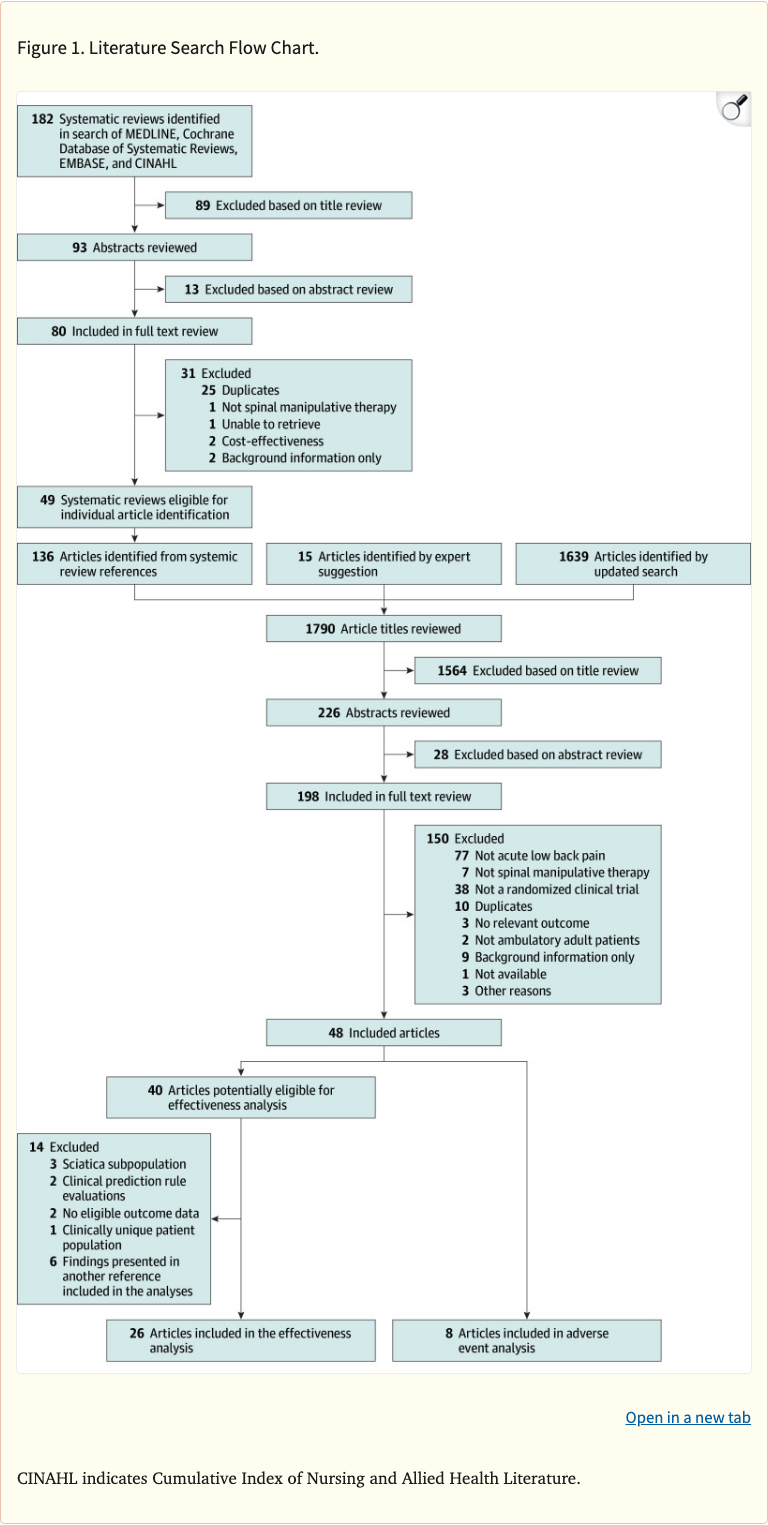 Figure 1
Figure 1
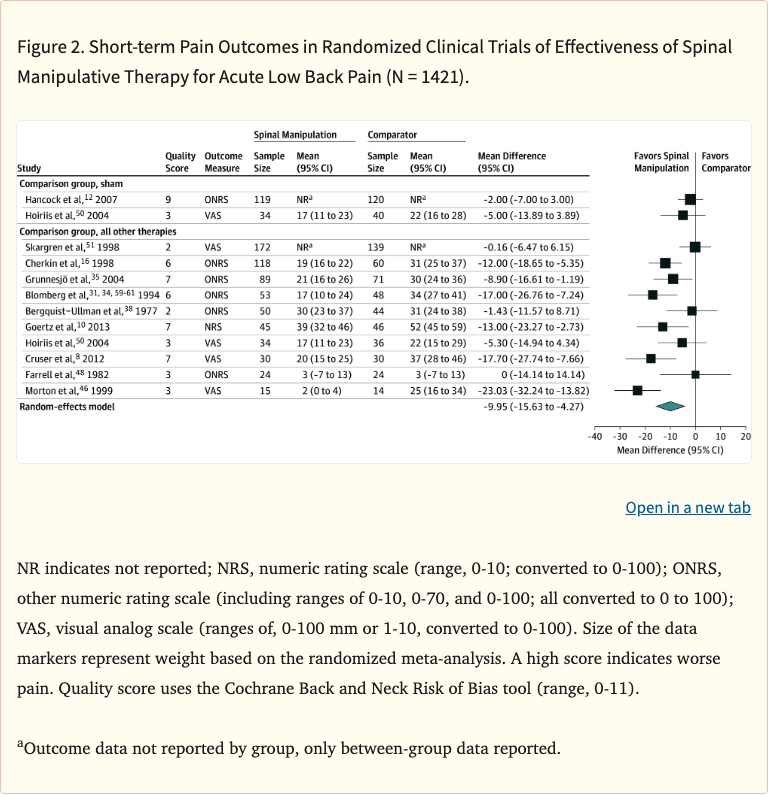 Figure 2
Figure 2
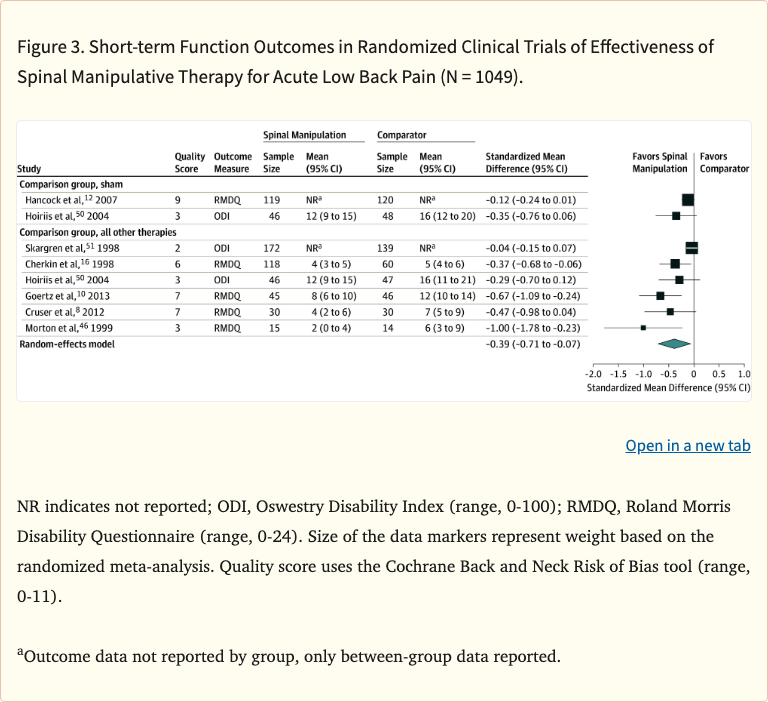 Figure 3
Figure 3
Limitations
Many included trials had methodological limitations including difficulty with blinding. Moderate to high heterogeneity in some analyses. Definition of "acute" low back pain varied across studies. Short follow-up in many trials. Comparison interventions varied widely. Quality of evidence was moderate at best. Clinical significance of ~10-point pain improvement debatable. Publication bias could not be excluded.