Key Takeaway
Network meta-analysis of 59 RCTs found live-high/train-low with low-altitude training is the most effective hypoxic protocol for VO2max improvement (P-score 0.86–0.92), with an inverted U-shaped dose-response curve.
Summary
This Bayesian network meta-analysis compared five types of hypoxic training interventions—live-high/train-high (LHTH), live-high/train-low (LHTL), live-high/train-high-low (HHL), intermittent hypoxic training (IHT), and intermittent hypoxic exposure (IHE)—on their ability to improve VO2max in athletes. From 2,072 identified titles, 59 randomized controlled trials were included in the final analysis.
The results showed that LHTL, LHTH, and IHT all significantly outperformed normoxic training for improving VO2max. Among all interventions, LHTL combined with low-altitude training (rather than sea-level training) was ranked as the most effective, whether using natural altitude (P-score 0.92) or simulated altitude (P-score 0.86). This was meaningfully better than LHTL with sea-level training (P-score 0.56).
A novel "kilometer hour" dosing model was used to standardize hypoxic exposure across different protocols. The dose-response analysis revealed an inverted U-shaped relationship for both LHTH (optimal range 470–1,130 kmh) and LHTL (optimal range 500–1,415 kmh), suggesting that both insufficient and excessive hypoxic exposure can impair performance gains. This finding has important practical implications for coaches designing altitude training camps.
Methods
Systematic search of Web of Science, PubMed, EMBASE, and EBSCO for RCTs published through February 2023. Bayesian network meta-analysis was used to compare five hypoxic training types. Hypoxic dosage was standardized using a "kilometer hour" (kmh) model that accounts for altitude and duration of exposure. P-scores were used to rank intervention effectiveness. Dose-response curves were fitted to examine the relationship between hypoxic dosage and VO2max changes.
Key Results
From 59 included RCTs, LHTL, LHTH, and IHT all significantly improved VO2max versus normoxic training. LHTL with low-altitude training was the most effective intervention (P-scores: natural 0.92, simulated 0.86), outperforming LHTL with sea-level training (P-score 0.56). An inverted U-shaped dose-response relationship was identified for LHTH (optimal: 470–1,130 kmh) and LHTL (optimal: 500–1,415 kmh). IHE alone did not significantly improve VO2max.
Figures
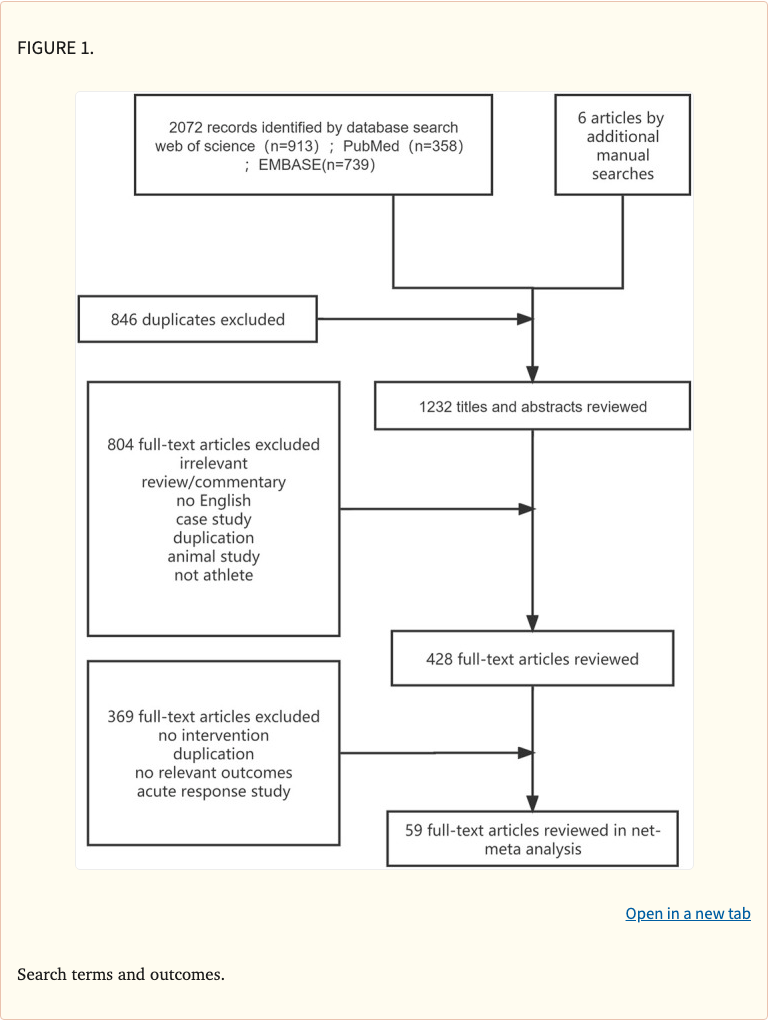 Figure 1
Figure 1
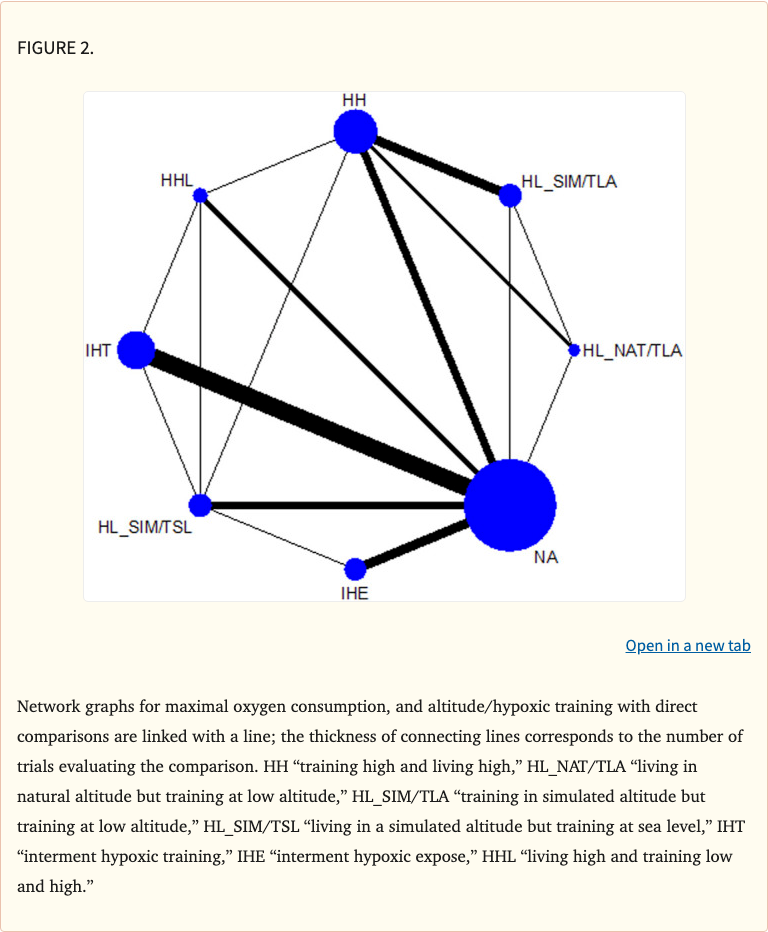 Figure 2
Figure 2
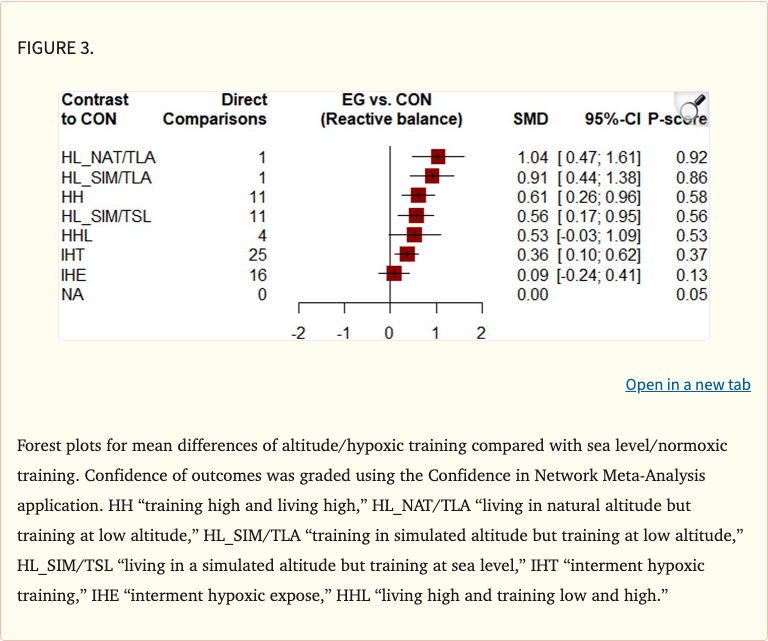 Figure 3
Figure 3
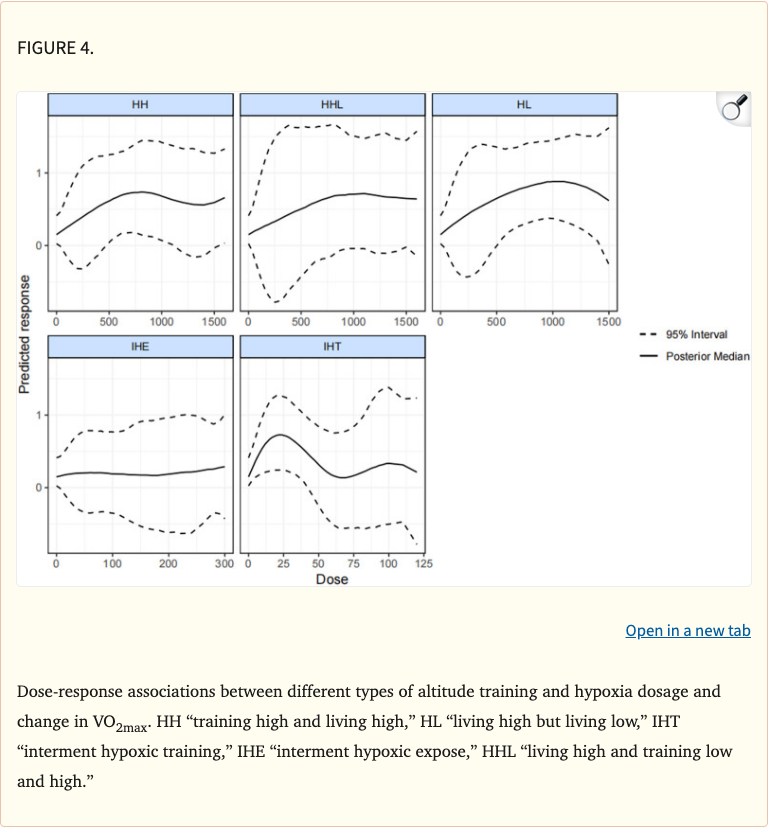 Figure 4
Figure 4
Limitations
Heterogeneity existed across studies in terms of athlete populations, sports, training intensities, and altitude levels. The "kilometer hour" dosing model, while useful for standardization, is a simplified representation of hypoxic stimulus. Some intervention subgroups had limited numbers of studies, potentially affecting ranking precision. Individual variation in altitude training response was not captured by the pooled analysis.