Key Takeaway
Each additional 1,000 daily steps reduces all-cause mortality risk by 12% and cardiovascular event risk by 5%, with benefits plateauing around 8,000-10,000 steps per day.
Summary
This dose-response meta-analysis examined the relationship between daily step count and both all-cause mortality and cardiovascular events. The authors synthesized data from prospective cohort studies to quantify how incremental increases in daily steps translate to measurable reductions in health risks.
The analysis found a clear nonlinear dose-response pattern: each 1,000-step increment was associated with a 12% reduction in all-cause mortality and a 5% reduction in cardiovascular events. The mortality benefit was most pronounced up to approximately 8,000-10,000 steps per day, after which the curve flattened but continued to show marginal improvements. For cardiovascular events, the protective association followed a similar pattern with steep initial gains that gradually diminished at higher step counts.
These findings reinforce that moderate daily walking targets (8,000-10,000 steps) capture the majority of the mortality and cardiovascular benefit, and that even modest increases in daily step count for sedentary individuals can produce clinically meaningful risk reductions.
Methods
Systematic search of PubMed, Embase, Web of Science, and Cochrane Library for prospective cohort studies reporting on daily step count and all-cause mortality or cardiovascular events. Dose-response relationships were modeled using restricted cubic splines. Study quality was assessed and heterogeneity was evaluated using standard meta-analytic methods.
Key Results
- Each additional 1,000 steps/day associated with 12% lower all-cause mortality risk (HR 0.88)
- Each additional 1,000 steps/day associated with 5% lower cardiovascular event risk (HR 0.95)
- Nonlinear dose-response: steepest risk reduction between 2,000-8,000 steps/day
- Benefits continued but plateaued beyond ~10,000 steps/day
- Consistent findings across subgroup analyses by age and sex
Figures
Limitations
- Observational design of included studies limits causal inference
- Step count measurement methods varied across studies (pedometers vs. accelerometers)
- Potential for residual confounding by overall physical activity level and fitness
- Limited data on cardiovascular events compared to mortality outcomes
- Most studies conducted in high-income Western populations, limiting generalizability
Related Interventions
Related Studies
Discussed In

Essentials: Tools to Boost Attention & Memory | Dr. Wendy Suzuki
Huberman Lab
Improve Your Lymphatic System for Overall Health & Appearance
Huberman Lab
How to Make Yourself Unbreakable | DJ Shipley
Huberman Lab
Transform Your Metabolic Health & Longevity by Knowing Your Unique Biology | Dr. Michael Snyder
Huberman Lab
Essentials: Effects of Fasting & Time Restricted Eating on Fat Loss & Health
Huberman Lab

5 daily habits of people who live longer
ZOE Science & Nutrition
How to Grow From Doing Hard Things | Michael Easter
Huberman Lab

Optimizing Daily Habits: Snacking, Movement, Light Exposure, and More Wellness Hacks LIFE Network: RAW Podcast #3
Ben Greenfield Life

How Long Can Humans Really Live… (with Dan Buettner) : 1393
The Human Upgrade
Transform Your Mental Health With Diet & Lifestyle | Dr. Chris Palmer
Huberman Lab
Transform Your Health by Improving Metabolism, Hormone & Blood Sugar Regulation | Dr. Casey Means
Huberman Lab
Overcoming Physical & Emotional Challenges | Coleman Ruiz
Huberman Lab
How to Enhance Focus and Improve Productivity | Dr. Cal Newport
Huberman Lab
How to Build Immense Inner Strength | David Goggins
Huberman Lab
How to Use Exercise to Improve Your Brain’s Health, Longevity & Performance
Huberman Lab

Episode 424: How Daily Walking Can Transform your Health
Naturally Nourished
The daily step count that cuts inflammation in half | Prof. Janet Lord
ZOE Science & Nutrition
TMHS 255: Reduce Body Fat & Increase Your Lifespan: The Surprising Benefits Of Walking
The Model Health Show

Brand New Research on The Radical Benefits of Walking for Lowering Cholesterol, Body Fat, and Glucose, and Improving Your Mental Clarity with Greg Mushen
Dhru Purohit Show

Step by Step: Unlocking the Power of Walking with Ethan Suplee
American Glutton

The Science Of Walking: The Benefits Of Walking In Nature, Walking Meetings, And Walking Meditation | Dacher Keltner
10% Happier with Dan Harris

Neuroscientist Reveals the Insane Benefits of Walking Everyday for Brain Health and Longevity with Shane O'Mara
Dhru Purohit Show

Born to Carry — How to Build Strength, Stamina, and Sanity Through Rucking
The Art of Manliness

Rucking for Women
Fuel Your Strength

Ep. #718: Here’s Why You Should Start Rucking (Especially If You Hate Cardio)
Muscle for Life with Mike Matthews
The Benefits of Rucking for Women w/ Michael Easter
Fuel Your Strength

Get Rucking
The Art of Manliness

#292 ‒ Rucking: benefits, gear, FAQs, and the journey from Special Forces to founding GORUCK | Jason McCarthy
The Peter Attia Drive
#713 Rage Rucking
Juicebox Podcast: Type 1 Diabetes
#314: Building Better Citizens Through Rucking
The Art of Manliness
Body of Health PODCAST 02 Rebounding
Tell Me Your Story

Rebounding vs Walking for Weight Loss | What Actually Works After 40 - 1272
The Chalene Show | Diet, Fitness & Life Balance

Walks, Hikes, and Loaded Carries
Autonomy by GMB Fitness

Ep. #896: Kyle Hunt on Underrated Exercises You Should Be Doing
Muscle for Life with Mike Matthews

Sled Training Benefits
Jeremy Scott Fitness

Menopause Weight Loss made simple | Does the 30 30 30 Rule actually work?
Golden Tails and Trails | Canicross Running and Weight loss for women | Lose weight, get fit and stay motivated through running and canicross with your dog
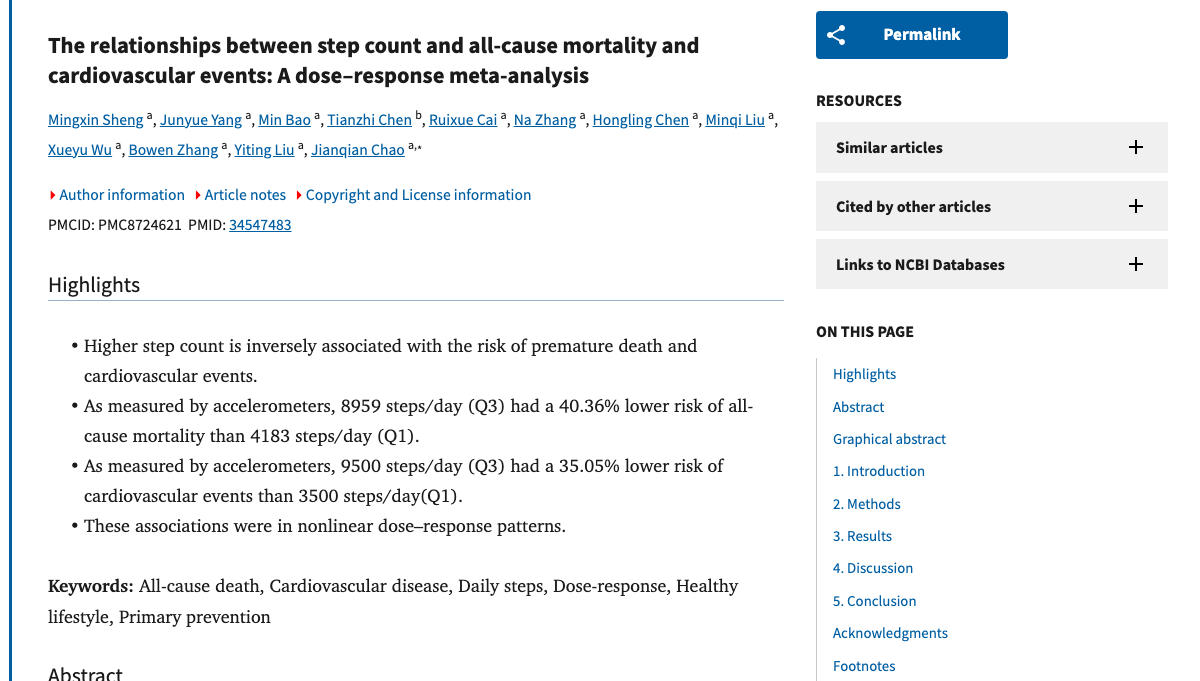
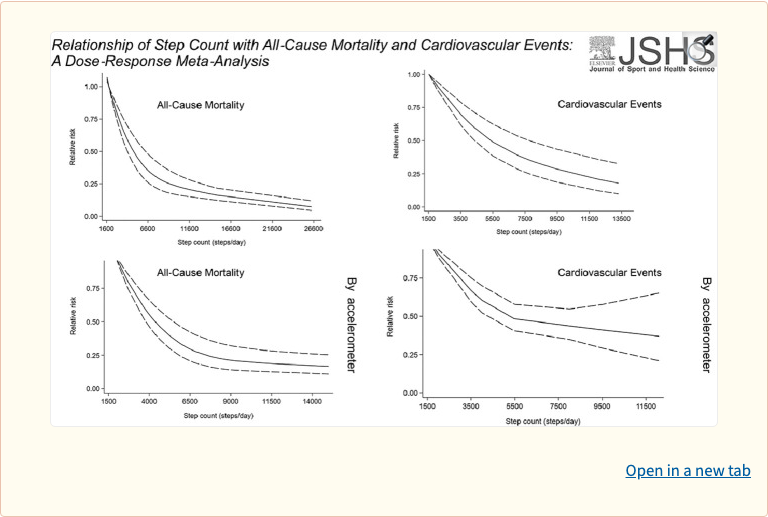 Figure 1
Figure 1
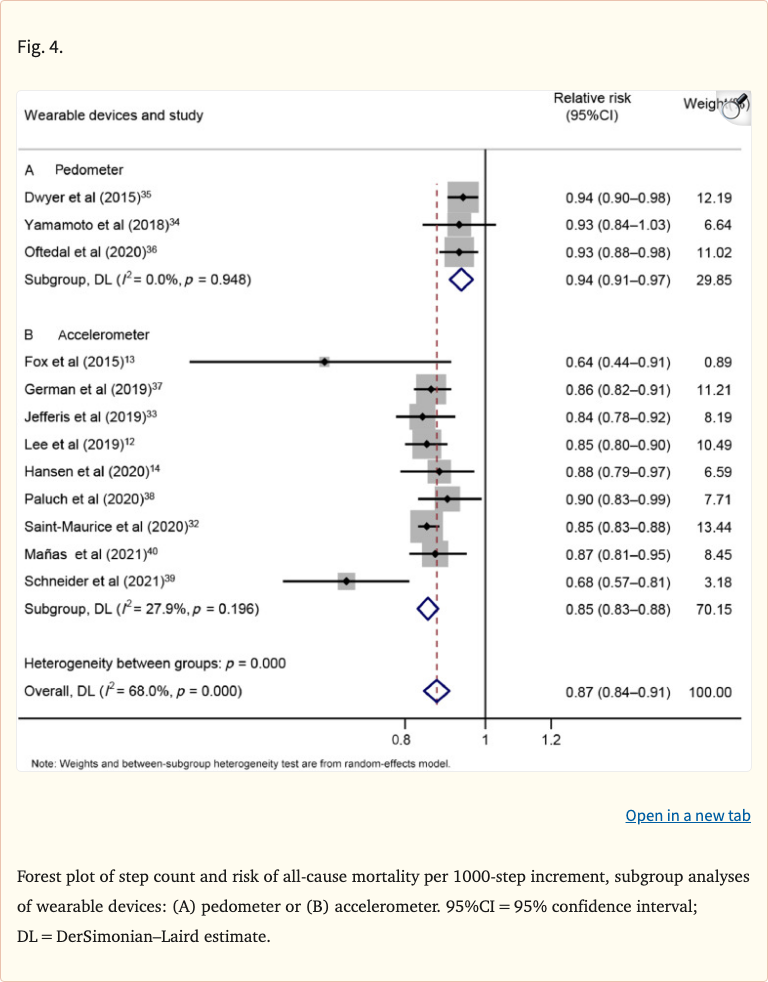 Figure 4
Figure 4
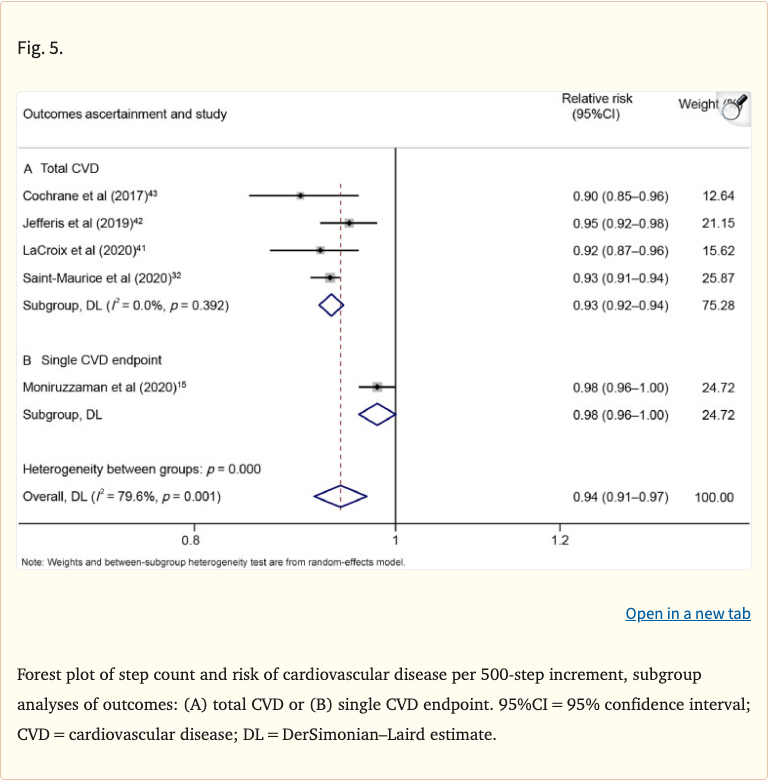 Figure 5
Figure 5