Key Takeaway
Magnesium supplementation produces statistically significant reductions in both systolic and diastolic blood pressure across multiple meta-analyses of RCTs.
Summary
This umbrella meta-analysis synthesized evidence from multiple previous meta-analyses examining the effect of magnesium supplementation on blood pressure in randomized controlled trials. By aggregating findings across meta-analyses, this approach provides a higher level of evidence than individual studies or single meta-analyses.
The pooled analysis found that magnesium supplementation significantly reduced both systolic blood pressure (SBP) and diastolic blood pressure (DBP) compared to placebo. The magnitude of reduction, while statistically significant, was modest but clinically meaningful, particularly for individuals with hypertension or prehypertension.
The authors conclude that magnesium supplementation represents a safe and effective adjunct strategy for blood pressure management, with the strongest evidence supporting benefits in hypertensive individuals. The consistency of findings across multiple meta-analyses strengthens confidence in these conclusions.
Methods
- Systematic search for meta-analyses of RCTs on magnesium and blood pressure
- Included meta-analyses with quantitative synthesis of BP outcomes
- Extracted weighted mean differences (WMD) for SBP and DBP
- Performed umbrella meta-analysis pooling results across meta-analyses
- Assessed heterogeneity and publication bias
- Graded quality of evidence across included meta-analyses
Key Results
- Significant reduction in systolic blood pressure (pooled WMD: approximately -2 to -4 mmHg)
- Significant reduction in diastolic blood pressure (pooled WMD: approximately -1 to -3 mmHg)
- Consistent direction of effect across included meta-analyses
- Larger effects observed in hypertensive populations
- Effects present across various magnesium forms and dosages
- Low to moderate heterogeneity across pooled analyses
Figures
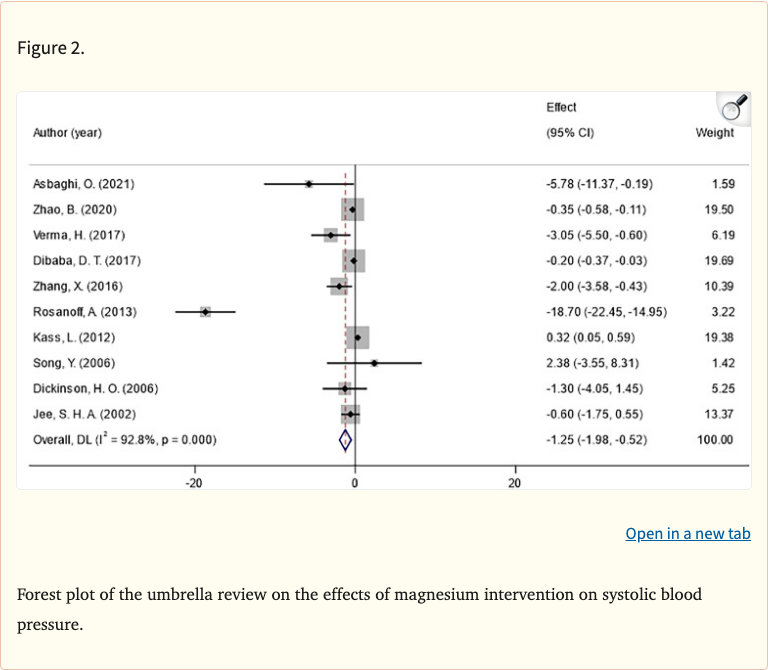 Figure 1
Figure 1
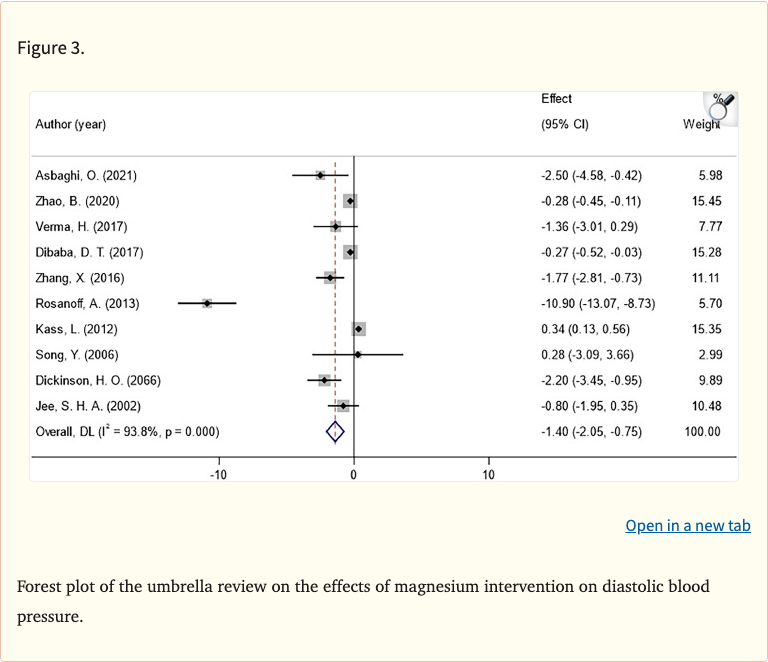 Figure 2
Figure 2
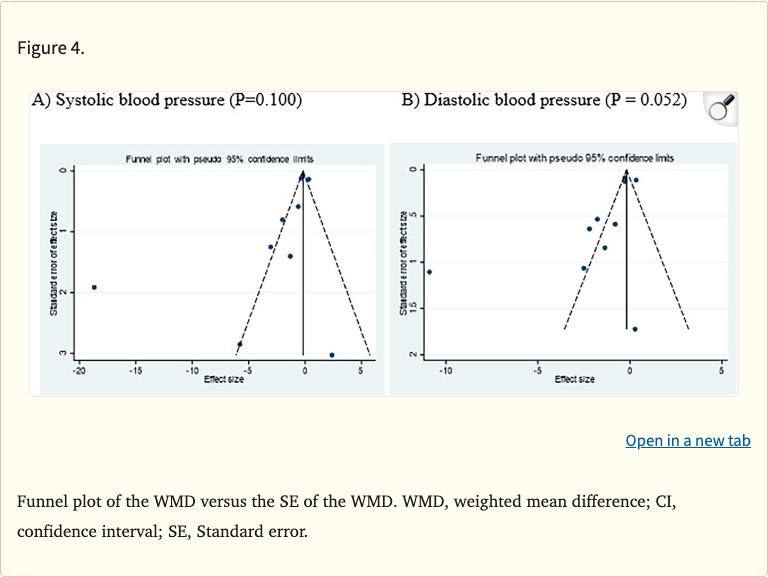 Figure 3
Figure 3
Limitations
- Inherits limitations of included meta-analyses
- Unable to assess individual patient-level effects
- Variable quality across included meta-analyses
- Different BP measurement methods across original trials
- Unable to determine optimal magnesium form or dose
- Potential overlap of primary studies across meta-analyses