Key Takeaway
Breathwork produces small-to-medium reductions in stress (g = -0.35), anxiety (g = -0.32), and depressive symptoms (g = -0.40) compared to non-breathwork controls across 12-20 RCTs.
Summary
This meta-analysis from researchers at the University of Sussex and University of Oxford is the first to examine the effects of breathwork specifically (not as part of broader yoga or mindfulness programs) on stress, anxiety, and depression. Searching seven databases through February 2022, the authors identified 26 RCTs meeting inclusion criteria, with breathwork comprising at least 50% of each intervention.
For the primary outcome of self-reported stress (12 RCTs, n=785), breathwork produced a significant small-to-medium effect (Hedges' g = -0.35, p = 0.0009) with moderate heterogeneity (I-squared = 42%). Secondary outcomes showed similar benefits for anxiety (20 studies, g = -0.32, p < 0.0001) and depression (18 studies, g = -0.40, p < 0.0001). Most included studies used slow-paced breathing techniques (10 of 12 stress studies), and effects were significant across both in-person and remote delivery formats.
Subgroup analyses found no significant differences by population health status, breathing technique type, or delivery mode. Notably, no dose-response relationship emerged between intervention duration or session frequency and effect sizes. The authors caution that most studies carried moderate risk of bias and urge careful interpretation, warning against "miscalibration between hype and evidence" while acknowledging breathwork as a promising low-cost mental health intervention.
Methods
- Searched 7 databases (PsycInfo, PubMed, ProQuest, Scopus, Web of Science, ClinicalTrials.gov, ISRCTN) through February 2022
- Included RCTs with breathwork comprising 50% or more of intervention, adult participants, and stress/anxiety/depression outcomes
- Excluded interventions requiring equipment to physically alter breathing
- 1,325 initial results screened; 26 reports included (12 for stress, 20 for anxiety, 18 for depression)
- Random-effects meta-analysis using Hedges' g standardized mean differences
- Heterogeneity assessed via Cochran's Q and Higgins' I-squared
- Publication bias examined with funnel plots and Egger's test
- Subgroup analyses by population, technique type, delivery mode, and control group type
Key Results
- Stress (primary, k=12, n=785): g = -0.35 (95% CI -0.55 to -0.14), p = 0.0009, I-squared = 42%
- Anxiety (k=20): g = -0.32, p < 0.0001, I-squared = 51%
- Depression (k=18): g = -0.40, p < 0.0001, I-squared = 58%
- No significant dose-response relationship between session frequency or duration and effect size
- Effects significant for both nonclinical (g = -0.34) and clinical populations
- Group delivery showed larger point estimate (g = -0.59) than individual (g = -0.26) but difference not significant
- Low publication bias (Egger's test z = 0.03, p = 0.947; fail-safe N = 69)
Figures
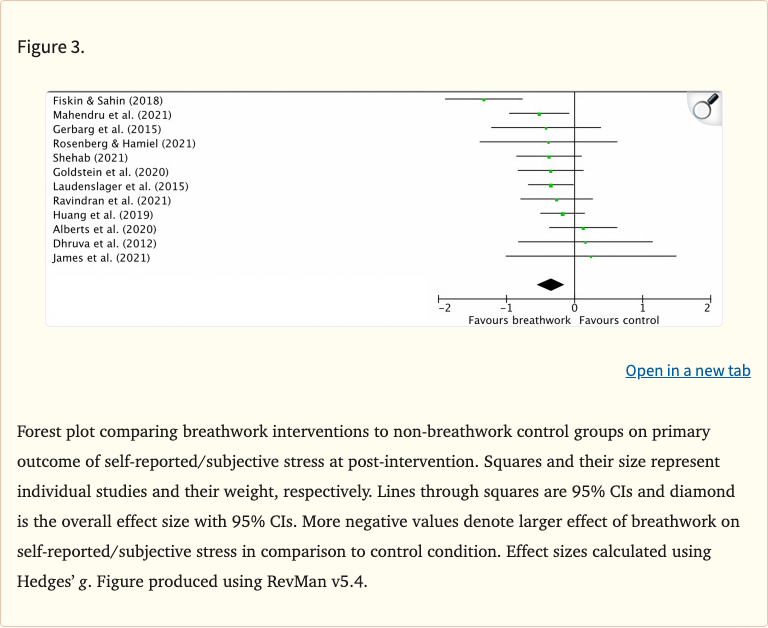 Figure 1
Figure 1
Limitations
- Most studies carried moderate risk of bias (3 high risk, 9 some concerns)
- Small sample sizes within individual studies (10-150 participants each)
- Insufficient follow-up data to assess long-term effects
- Reliance on self-report outcome measures without objective physiological markers
- Significant heterogeneity in anxiety and depression outcomes suggests unmeasured moderators
- Limited home practice compliance reporting prevented true dose-response analysis
- 60% of included stress studies published from 2020 onward, reflecting a young evidence base