Key Takeaway
Meta-analysis of 38 RCTs (2,472 participants) found neurofeedback did not significantly improve ADHD symptoms under probably-blinded assessment (SMD = 0.04), though standard protocols showed a small effect (SMD = 0.21).
Summary
This systematic review and meta-analysis, published in JAMA Psychiatry by the European ADHD Guidelines Group, evaluated the efficacy of neurofeedback for treating ADHD by analyzing 38 randomized clinical trials encompassing 2,472 participants aged 5 to 40 years. The study focused specifically on probably-blinded outcome assessments — reports from individuals judged to be unaware of treatment allocation — to reduce placebo and expectation bias.
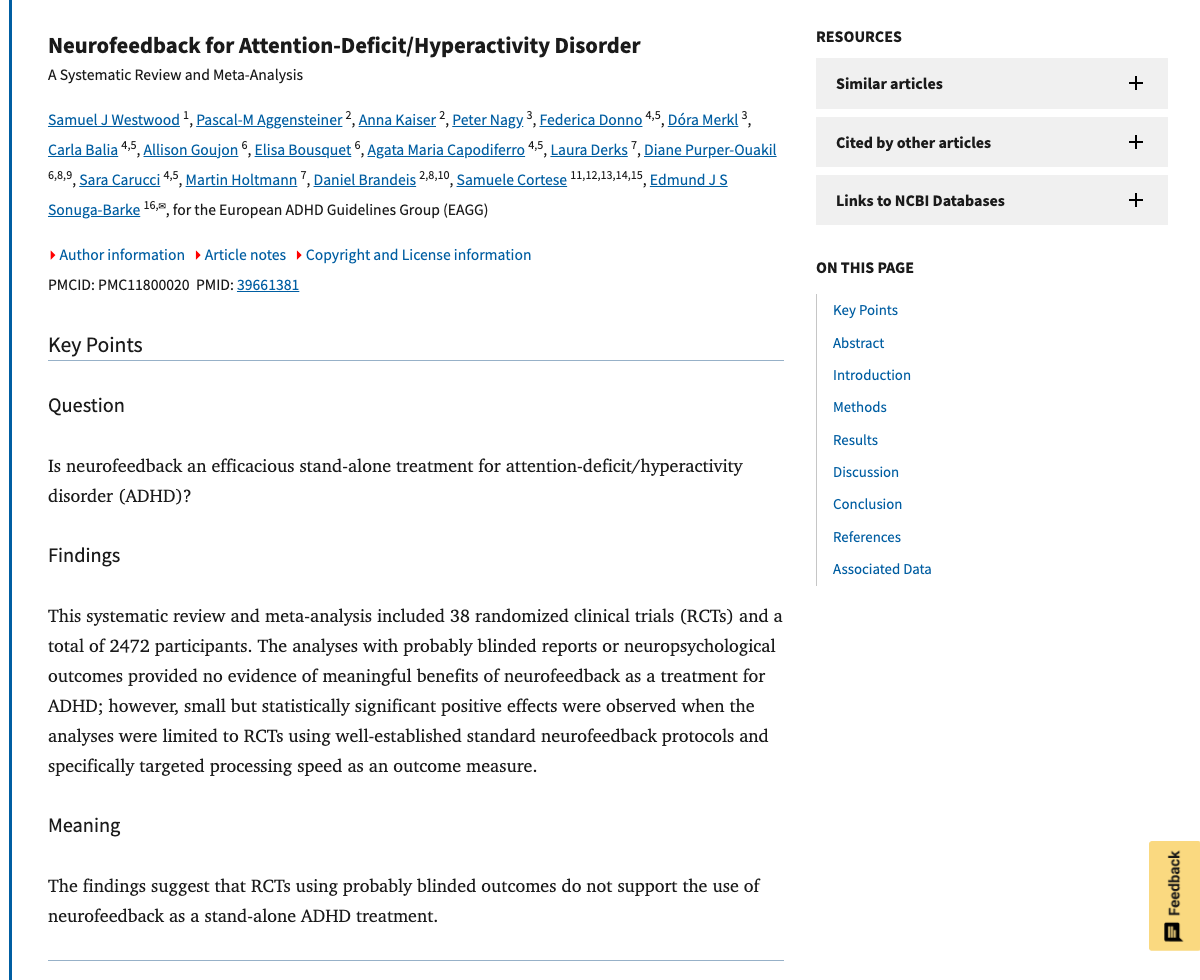
The primary analysis found no significant improvement in ADHD total symptoms when assessed by probably-blinded raters (SMD = 0.04, 95% CI: -0.10 to 0.18). However, a subgroup analysis restricted to RCTs using established standard neurofeedback protocols (such as theta/beta ratio or sensorimotor rhythm training) showed a small but statistically significant effect (SMD = 0.21, 95% CI: 0.02 to 0.40). Among five neuropsychological outcomes analyzed, only processing speed showed a significant improvement (SMD = 0.35).
The authors conclude that neurofeedback does not appear to meaningfully benefit individuals with ADHD at the group level, and suggest that future research should focus on identifying specific patient subgroups who may respond, using standard protocols, and leveraging precision medicine approaches.
Methods
Systematic review and meta-analysis of parallel-arm RCTs investigating neurofeedback in participants with clinical ADHD diagnoses. Databases searched included PubMed, Ovid (PsycInfo, MEDLINE, Embase), and Web of Science through July 2023. Standardized mean differences (SMDs) with Hedges' g correction were pooled using random-effects models. The primary outcome was ADHD total symptom severity assessed by probably-blinded raters. Risk of bias was assessed using Cochrane RoB 2.0.
Key Results
Probably-blinded ADHD total symptom ratings showed no significant effect of neurofeedback (k = 20, n = 1,214; SMD = 0.04, 95% CI: -0.10 to 0.18). Standard protocol RCTs showed a small significant effect (k = 9, n = 681; SMD = 0.21, 95% CI: 0.02 to 0.40). Among neuropsychological outcomes, only processing speed improved significantly (k = 15, n = 909; SMD = 0.35, 95% CI: 0.01 to 0.69). Heterogeneity was generally low to moderate across analyses.
Figures
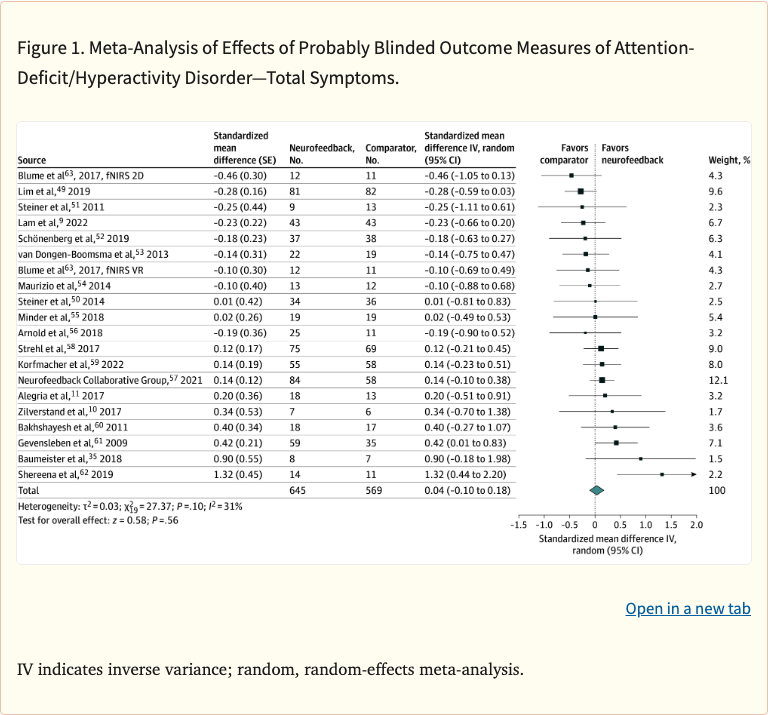 Figure 1
Figure 1
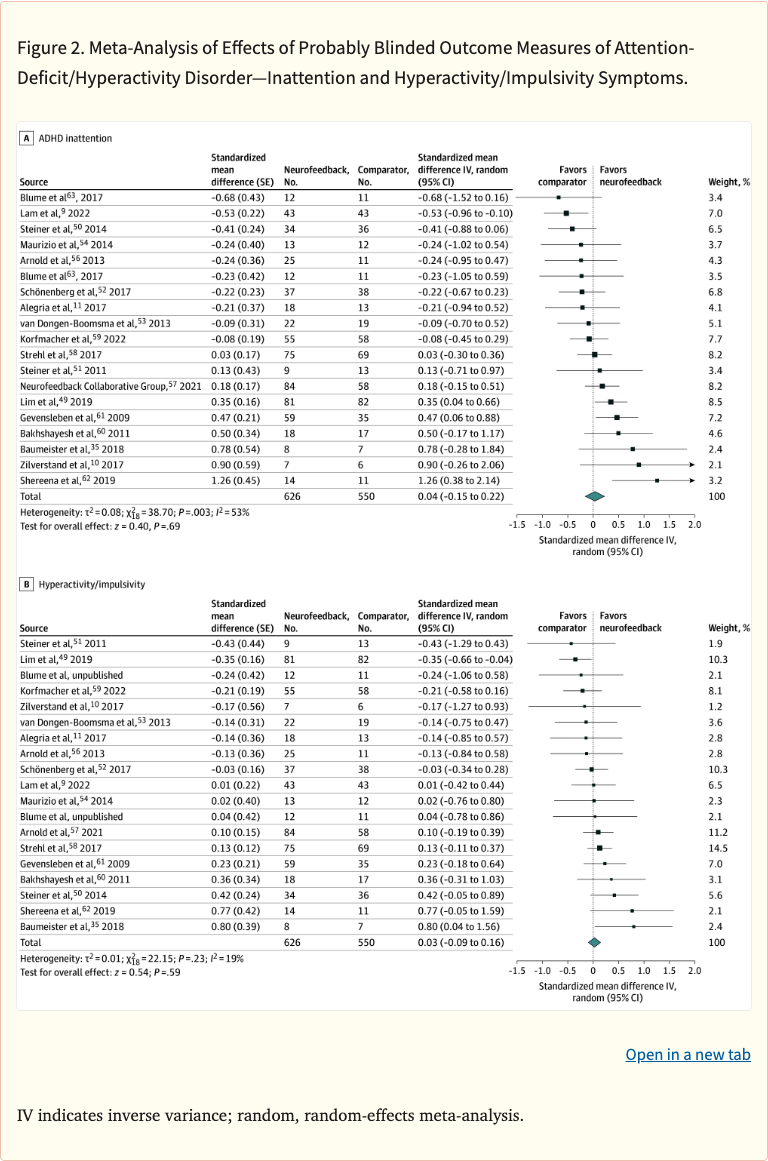 Figure 2
Figure 2
Limitations
Many included RCTs had small sample sizes and varied in neurofeedback protocols, session counts, and control conditions. The probably-blinded assessment requirement, while methodologically rigorous, reduced the number of eligible studies for the primary analysis. The meta-analysis could not fully account for individual differences in cortical learning capacity that may moderate treatment response.