Key Takeaway
Meta-analysis found weak handgrip strength associated with 95% increased risk of all-cause mortality in coronary artery disease patients (RR: 1.95), highlighting grip strength as a key prognostic marker in cardiac populations.
Summary
This meta-analysis investigated the association between handgrip strength and mortality outcomes specifically in patients with coronary artery disease (CAD). By focusing on this high-risk cardiac population, the study addressed whether grip strength—already established as a mortality predictor in general populations—holds similar or even stronger prognostic value for people with existing heart disease. Pooling data from multiple observational studies, the authors found that weak handgrip strength was associated with a 95% increase in all-cause mortality risk among CAD patients (RR: 1.95). Subgroup analyses confirmed the association held across different follow-up durations, geographic regions, and measurement methods. These results suggest that handgrip strength testing could serve as a simple, inexpensive screening tool in cardiac rehabilitation and cardiology clinics to identify patients at elevated mortality risk who might benefit from targeted strength training interventions.
Methods
Systematic review and meta-analysis following PRISMA guidelines. Searched PubMed, Embase, Cochrane Library, and Web of Science for studies examining handgrip strength and mortality in CAD patients. Included prospective cohort studies reporting hazard ratios or relative risks. Used random-effects models for pooled estimates. Performed subgroup analyses by follow-up duration, geographic region, sample size, and adjustment for confounders. Assessed heterogeneity with I-squared statistics and publication bias with funnel plots and Egger's test.
Key Results
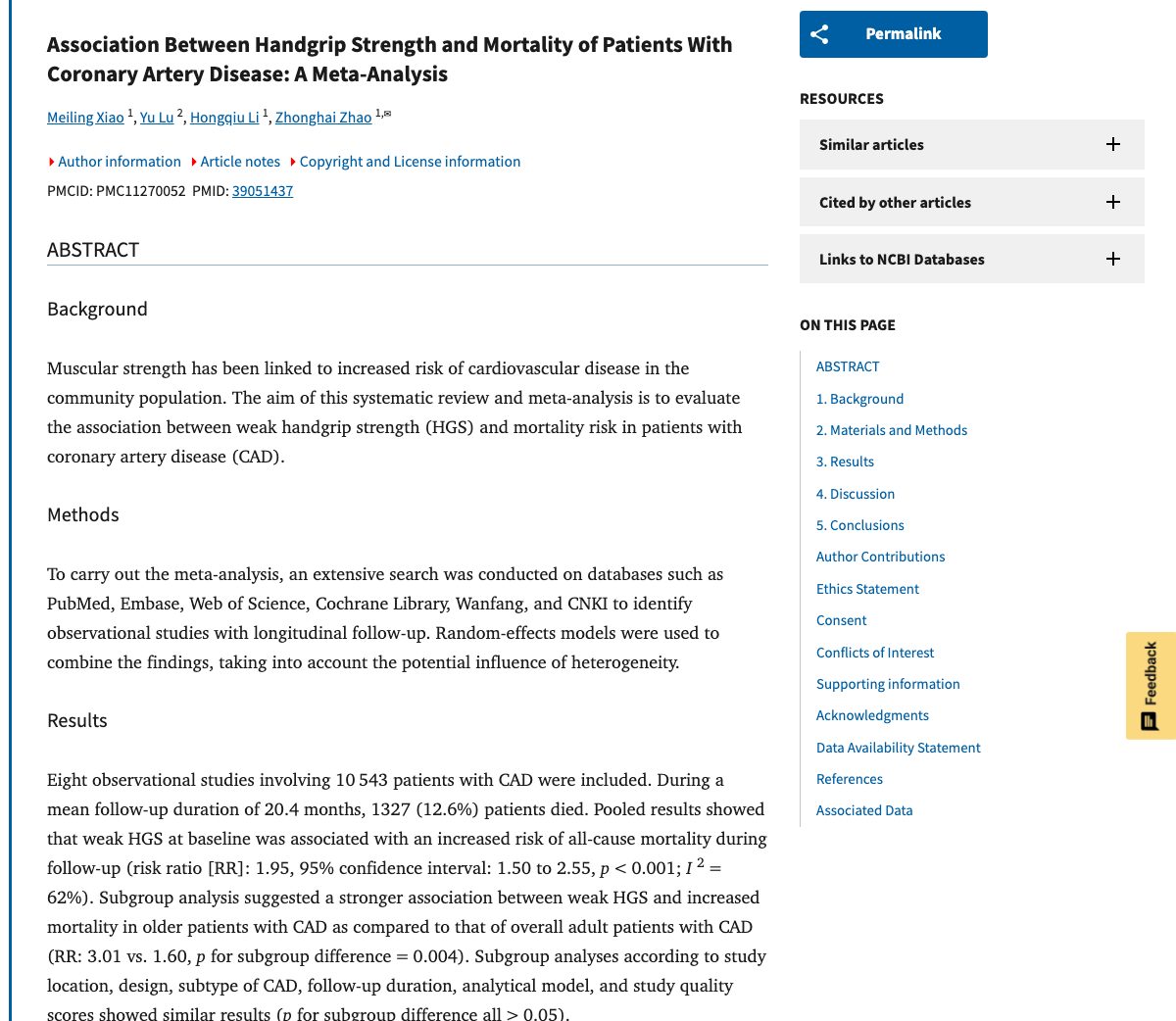
- Weak handgrip strength associated with 95% increased all-cause mortality risk in CAD patients (RR: 1.95)
- Association remained significant across all subgroup analyses
- Consistent findings regardless of follow-up duration (short-term and long-term)
- Results held across different geographic regions and study populations
- Low to moderate heterogeneity across included studies
- No significant publication bias detected
Figures
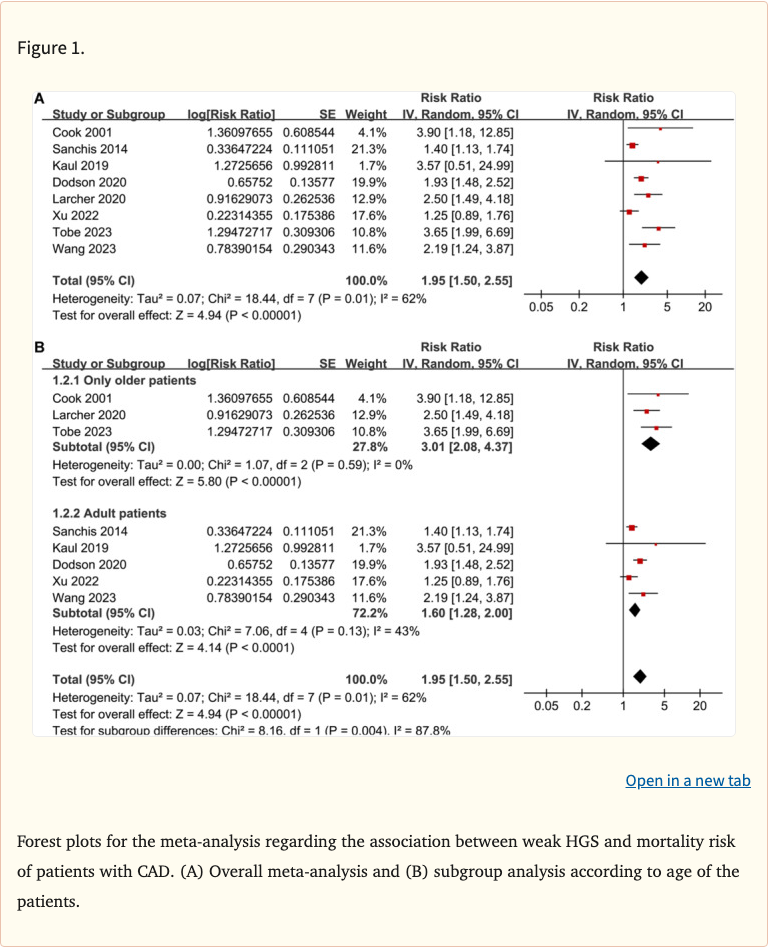 Figure 1
Figure 1
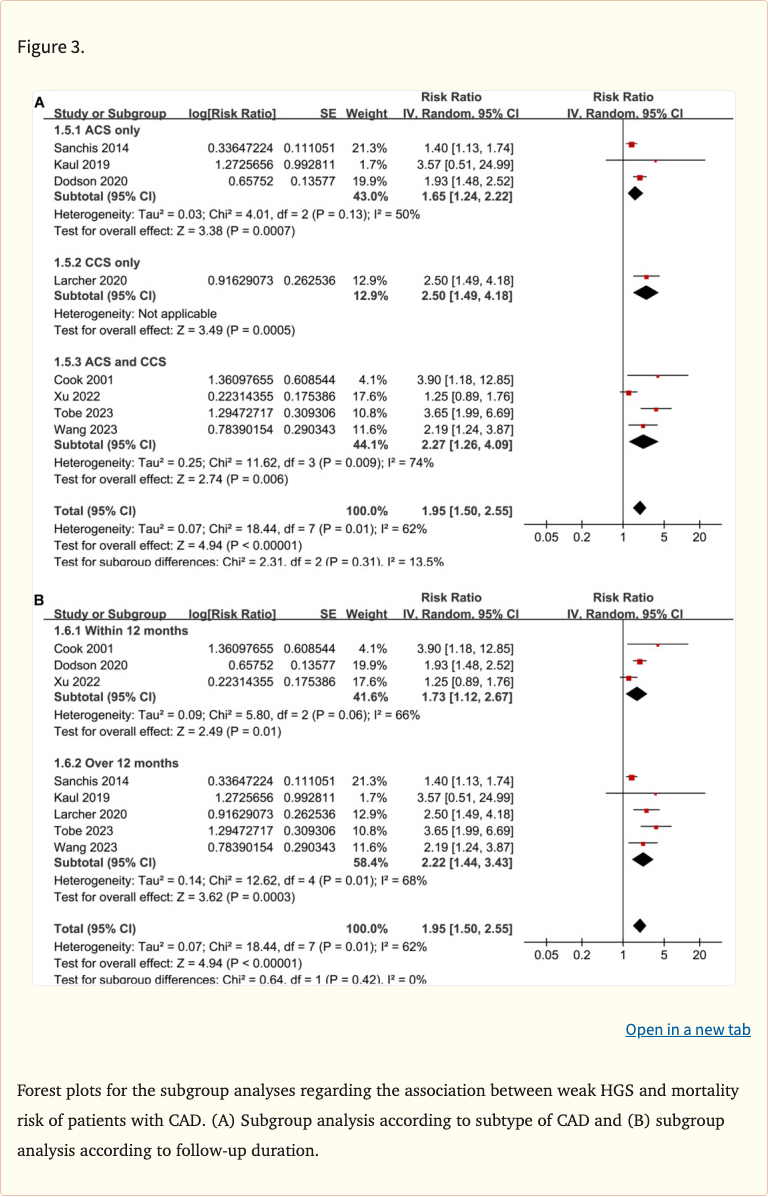 Figure 2
Figure 2
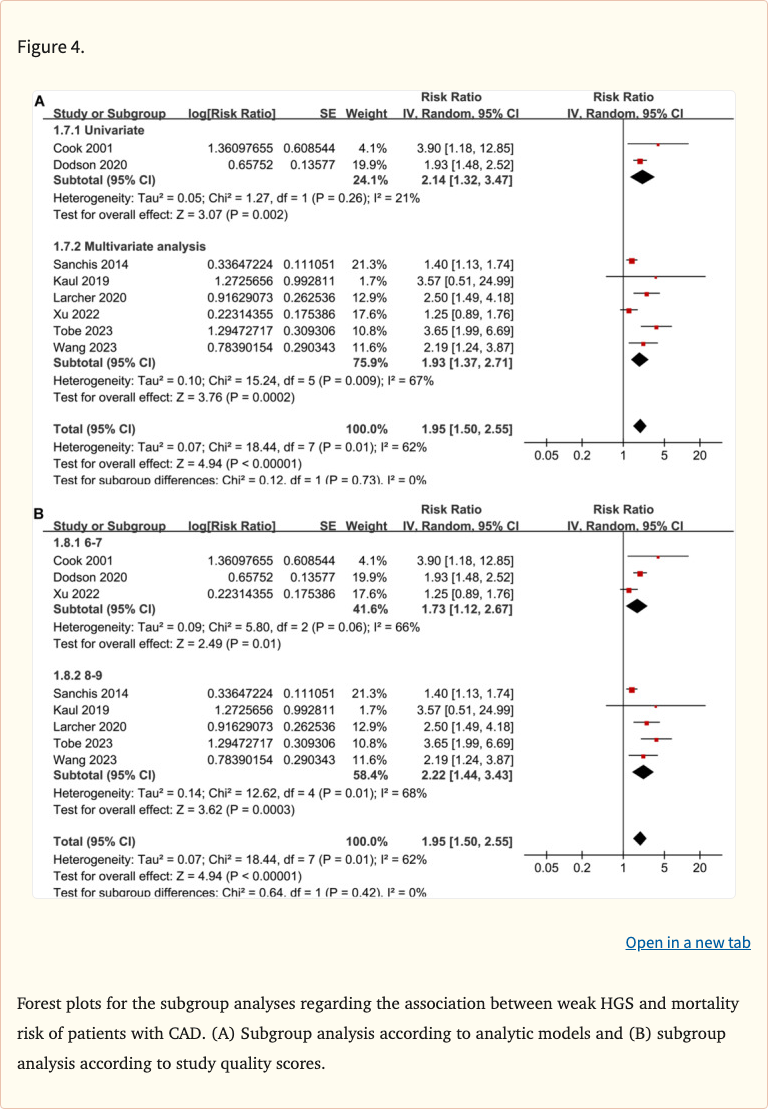 Figure 3
Figure 3
Limitations
- All included studies were observational, precluding causal conclusions
- Definitions of "weak" handgrip strength varied across studies
- Could not fully rule out reverse causation (sicker patients having weaker grip)
- Limited ability to assess whether improving grip strength would reduce mortality
- Most studies adjusted for different sets of confounders
- Relatively small number of included studies focused specifically on CAD populations