
Key Takeaway
Qigong significantly reduces systolic blood pressure by 10.66 mmHg and diastolic blood pressure by 6.76 mmHg compared to controls, with trial sequential analysis confirming sufficient evidence.
Summary
This systematic review and meta-analysis evaluated the effects of qigong exercise on blood pressure reduction, incorporating trial sequential analysis (TSA) to assess whether the cumulative evidence was conclusive.
Seven randomized controlled trials involving 370 participants were included. The pooled results demonstrated significant reductions in both systolic blood pressure (weighted mean difference -10.66 mmHg, 95% CI -17.69 to -3.62, p < 0.001) and diastolic blood pressure (weighted mean difference -6.76 mmHg, 95% CI -12.22 to -1.30, p < 0.001) in the qigong group compared to controls.
The trial sequential analysis, performed for the first time in qigong blood pressure research, confirmed that the cumulative Z-curve crossed the monitoring boundary for systolic blood pressure, suggesting the evidence is sufficient and conclusive. This strengthens the case for qigong as a complementary therapy for hypertension management.
The magnitude of blood pressure reduction observed (approximately 11/7 mmHg) is clinically meaningful and comparable to some first-line antihypertensive medications at low doses.
Methods
- Systematic search across Medline, Cinahl, Cochrane Central, and PubMed
- Seven eligible RCTs included (370 total subjects)
- Meta-analysis using random-effects model
- Trial sequential analysis to assess evidence conclusiveness
- Risk of bias assessment using Cochrane RoB 2 tool
Key Results
- Systolic BP reduction: -10.66 mmHg (95% CI -17.69 to -3.62, p < 0.001)
- Diastolic BP reduction: -6.76 mmHg (95% CI -12.22 to -1.30, p < 0.001)
- TSA confirmed sufficient evidence for systolic BP reduction
- Consistent direction of effect across included studies
- No significant publication bias detected
Figures
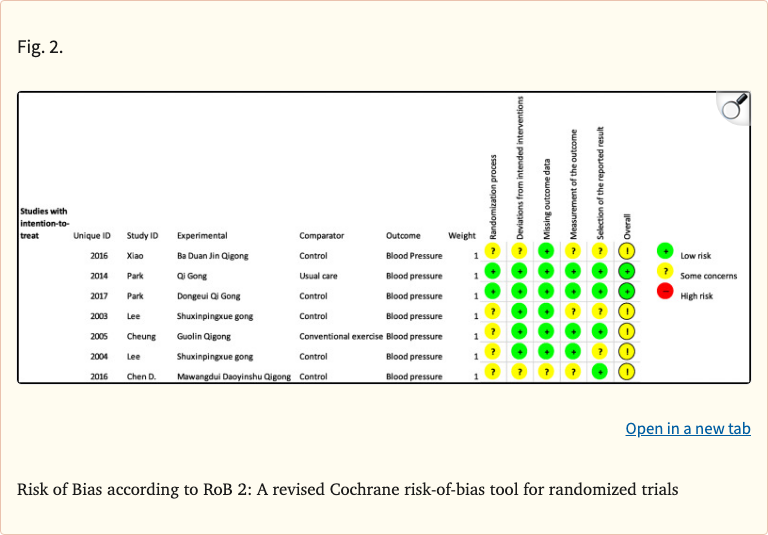 Figure 1
Figure 1
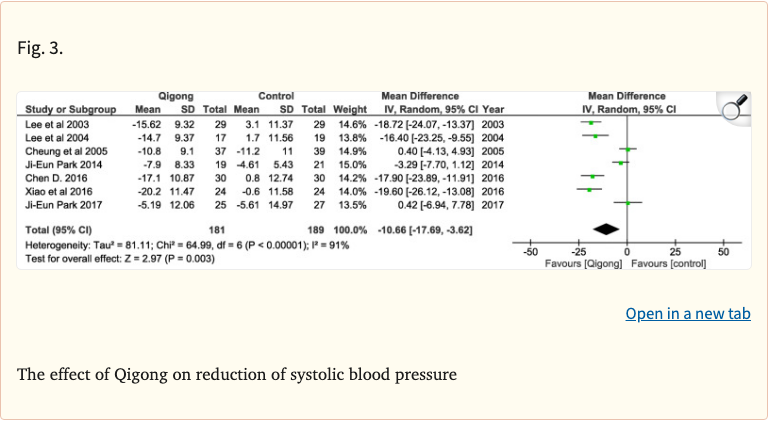 Figure 2
Figure 2
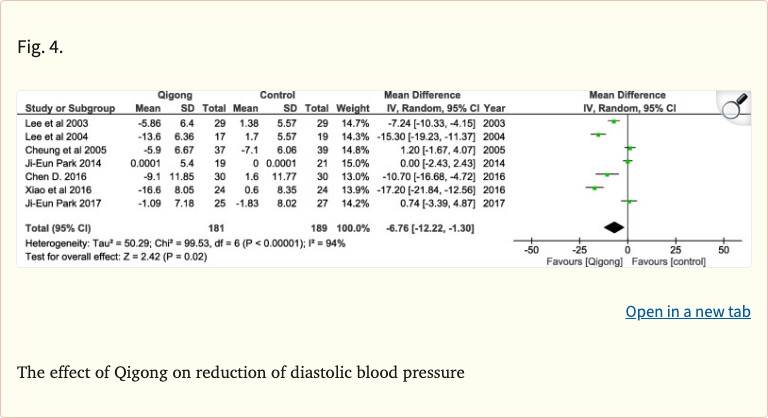 Figure 3
Figure 3
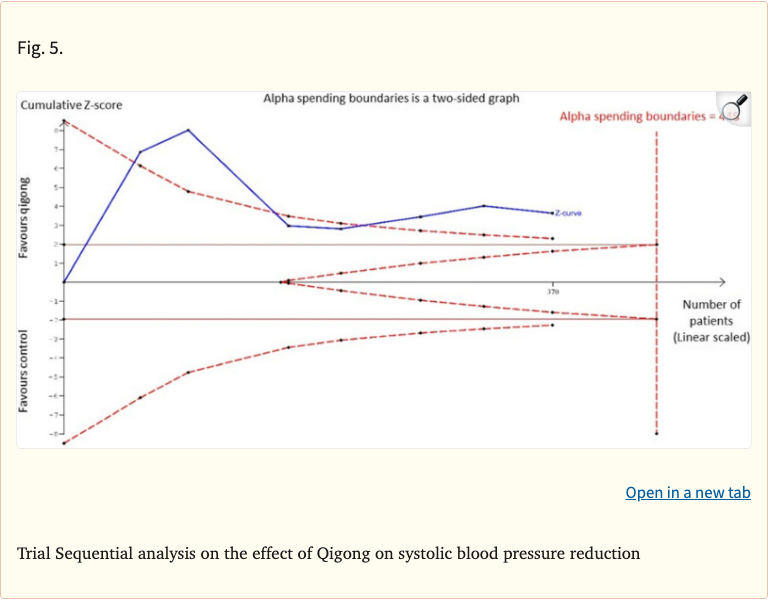 Figure 4
Figure 4
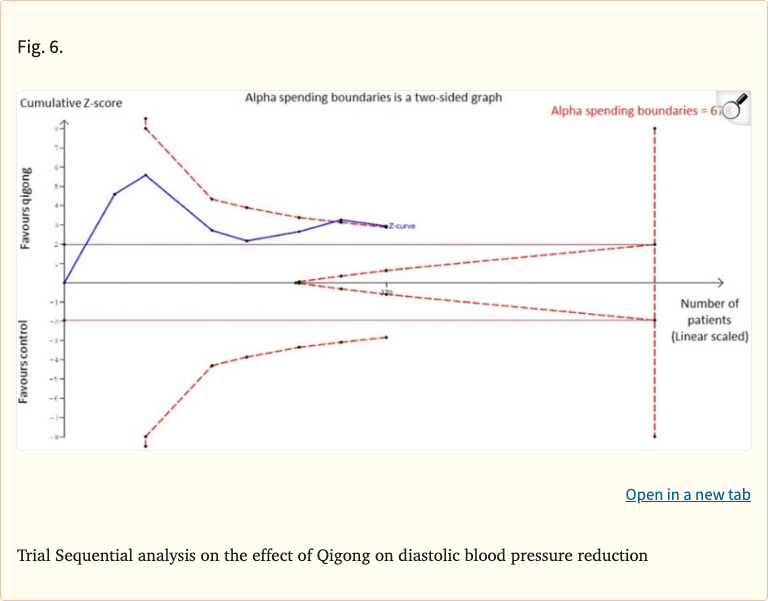 Figure 5
Figure 5
Limitations
- Small total sample size (370 participants across 7 RCTs)
- Heterogeneity in qigong styles and intervention duration
- Most studies from Asian populations, limiting generalizability
- Lack of long-term follow-up data
- Variable control conditions across studies