Key Takeaway
Mouth closure (via lip taping) during sleep reduced oral airflow and AHI in a subset of OSA patients, particularly those with higher baseline oral breathing.
Summary
This nonrandomized clinical trial published in JAMA Otolaryngology investigated the effects of mouth closure on airflow patterns and sleep apnea severity in patients with obstructive sleep apnea. The study used a novel approach to measure both nasal and oral airflow simultaneously during polysomnography, comparing breathing patterns with and without mouth closure achieved through lip taping.
The researchers found that responses to mouth closure were highly variable among participants. Patients who had higher baseline oral airflow (mouth breathers) tended to benefit most from mouth closure, showing reductions in oral airflow and improvements in AHI. However, patients who were already predominantly nasal breathers did not experience significant changes, confirming that the intervention specifically targets the mouth-breathing phenotype.
The study provides important objective data on the mechanism by which mouth taping may improve sleep apnea — by redirecting airflow through the nasal passages, which offer greater airway stability than the oral route. The findings suggest mouth closure could serve as a simple, low-cost adjunctive therapy for appropriately selected OSA patients, though individual assessment of breathing route is important for predicting response.
Methods
Nonrandomized clinical trial with crossover design. Patients with diagnosed OSA underwent overnight polysomnography with simultaneous measurement of nasal and oral airflow using partitioned oronasal masks. Each participant was studied under two conditions: baseline (mouth open) and mouth closure (achieved with lip tape). AHI, oral airflow fraction, and other respiratory parameters were compared between conditions.
Key Results
Mouth closure significantly reduced oral airflow in participants. Among responders (those with higher baseline oral airflow), AHI decreased with mouth closure. Nasal breathers at baseline showed minimal changes with mouth closure, confirming the phenotype-dependent nature of the intervention. The study identified that the degree of baseline oral breathing predicted the magnitude of improvement with mouth closure, providing a potential biomarker for patient selection.
Figures
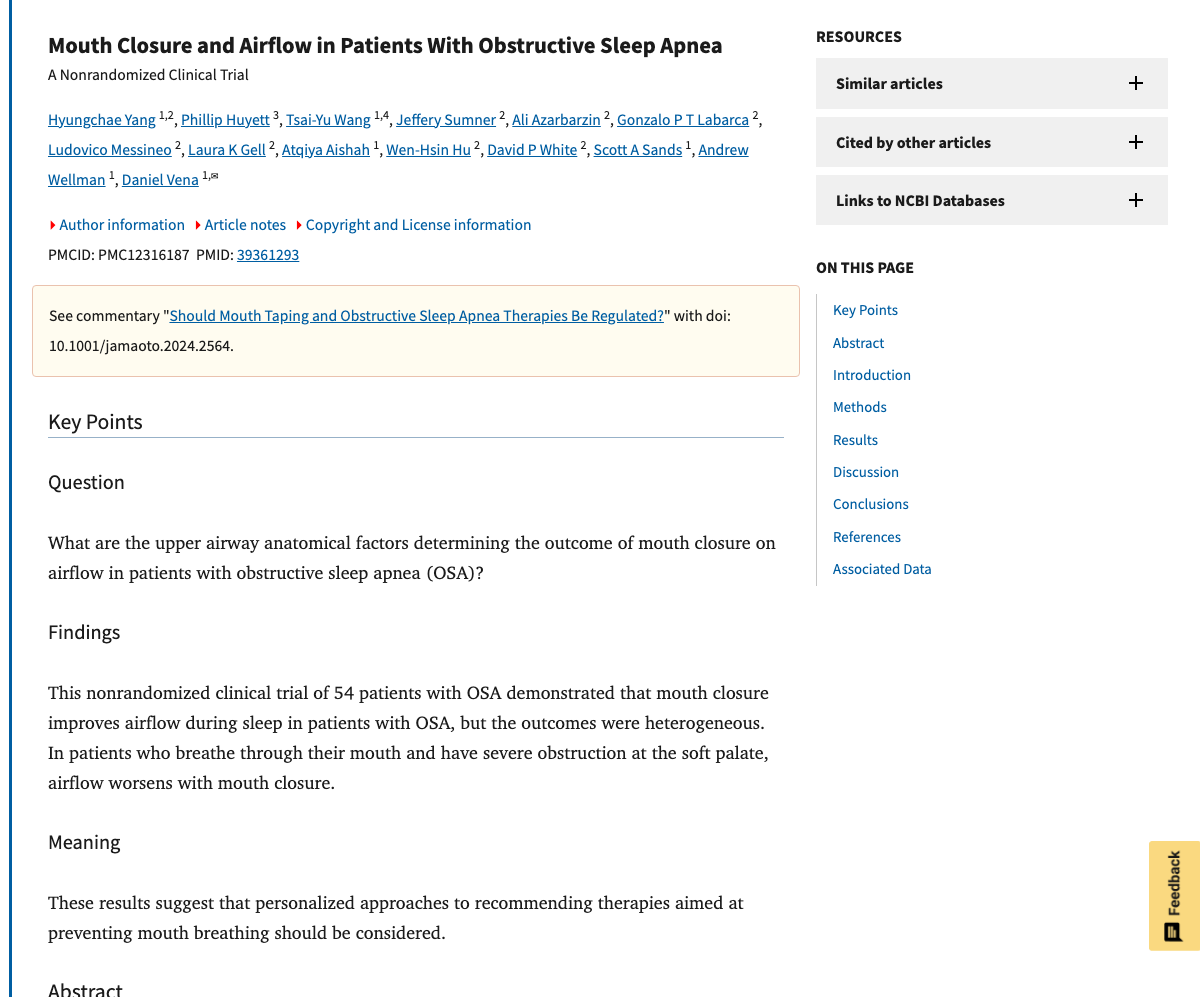
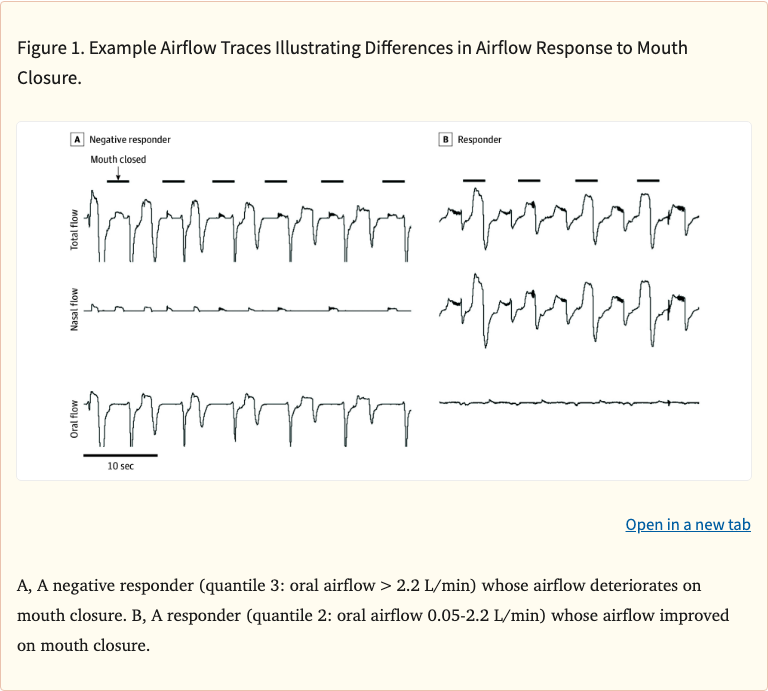 Figure 1
Figure 1
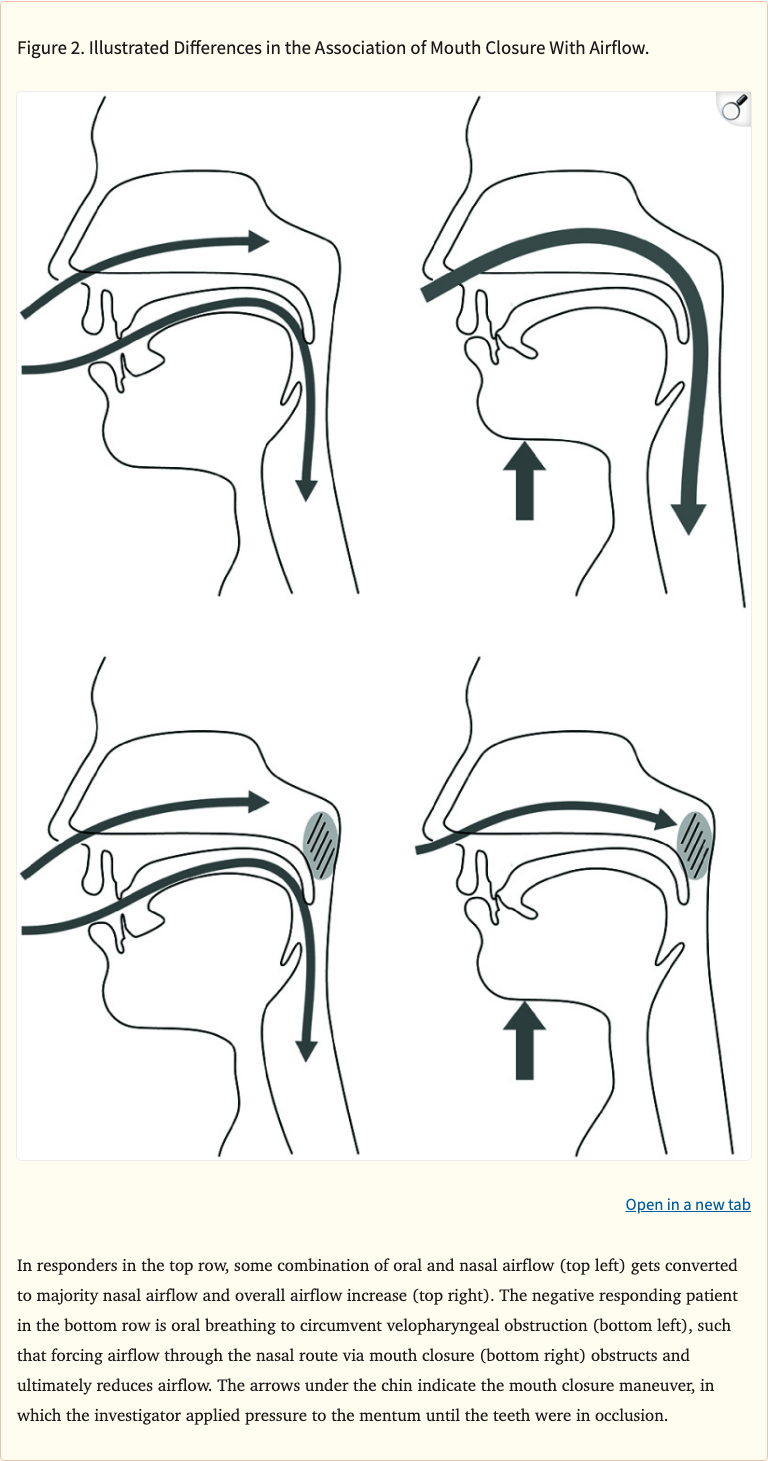 Figure 2
Figure 2
 Figure 3
Figure 3
Limitations
The study used a nonrandomized design, which limits causal inference. The sample size was relatively small. The lip taping method used in the controlled lab setting may not perfectly replicate real-world mouth taping during sleep. Only a single night of data was collected per condition, which may not capture night-to-night variability. Long-term adherence and outcomes were not assessed.